
About Kidney Problems - nephrologist or urologist?
Nephrologists are concerned with any disease that affects kidney function
This is usually manifest as an abnormal finding in a blood test, protein in the urine and/or high blood pressure: details of these are found throughout this website.
In general though, if a surgical solution is likely then a urologist should be consulted. Even then, a nephrologist will be able to perform baseline investigations and refer on as appropriate. Areas of overlap include haematuria (blood in the urine), kidney stones, recurrent urine infection and kidney pain. In addition, if a urologist needs to remove a substantial amount of kidney tissue (for cancer for example) then a nephrologist should be involved. David works closely with urologists so you can be assured of seamless care.
Haematuria (blood in urine): there are clear guidelines about whom to consult when blood in the urine is found. For guidance click here.
Kidney stones: this is usually dealt with by urologists although
investigations for susceptibility to stones, advice for the prevention of stones and some medical treatments to prevent stone formation can be provided by a nephrologist. For more information click
here.
Recurrent urine infection: this is a common problem of both specialties and
most cases do not require a surgical solution. A nephrologist can investigate and advise on treatment for this problem. If investigations suggest a urological solution then a referral is easily
arranged.
Kidney pain: this is a difficult problem. Most pain experienced over the kidney
area ( at the back beneath the ribs) is actually coming from the bones, muscles or nerves around the spine and has nothing to do with the kidneys at all. Conditions that cause haematuria can cause
kidney pain as can kidney stones and blockage of urine outflow and other rare conditions. Either specialist is able to investigate whether kidney pain is likely to originate from the kidneys and
advise accordingly.
Chronic Kidney Disease (CKD)
 Stages of CKD
Stages of CKD
Just to be clear, a "chronic" problem is one that has been going on a long time: the word does not refer to severity. Indeed most cases of chronic kidney disease (CKD) are mild.
The concept of CKD was developed in 2001/02 when it was becoming clear that a lot of people had a significant reduction in kidney function which traditional blood tests taken in isolation were
failing to detect. This led to numerous formulae which more accurately measure kidney function and this has been adopted worldwide.
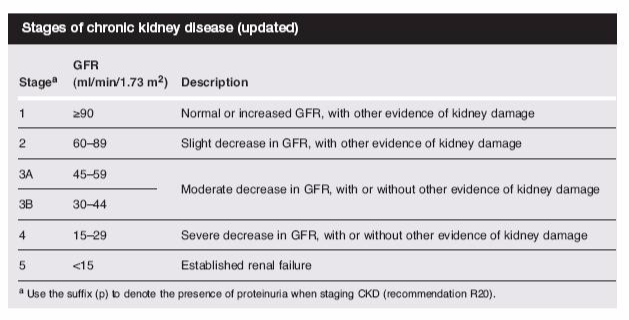
Kidney function is measured by glomerular filtration rate (GFR) which roughly approximates to percentage kidney function. Chronic kidney disease has been divided into stages as shown in the table
above. For a GFR calculator click here.
There are 2 important things to bear in mind when looking at this table. The first is that the accuracy of the percentage prediction in CKD3 or better is poor. Therefore if your doctor tells you that you have CKD3 and this is stable then don't worry: control of blood pressure and other lifestyle interventions are likely to be all that is required.
NHS Recommendations for when to refer to a nephrologist can be found here.
The second thing to consider is that dialysis treatment in the UK is required, on average, when the kidneys are working at 8%. So although being told that your kidneys are working at 35% might be
worrying, dialysis (or transplantation) is unlikely to ever be needed for most people with CKD3.
It is the job of the nephrologist to try to ensure that useful kidney function is sustained as long as possible but that if dialysis or transplantation are likely to be needed then this is planned
for in a timely fashion.
Please note that although most Health Insurance companies will reimburse initial investigation and management of CKD, they do not support ongoing CKD management beyond a few years (please check), nor
dialysis and transplantation.
For more details on CKD click here.
One of the commonest causes of CKD in the UK is diabetic kidney disease (or diabetic nephropathy). This usually occurs over many years and is initially manifest by small amounts of protein in the
urine, then more protein, and then a decline in kidney function. In common with most other causes of CKD, most patients with diabetic kidney disease will not need dialysis or a kidney transplant. The
role of the nephrologist is to maximise a patient's chances of not needing these, by preserving kidney function as long as possible. Dr Game is experienced in treating diabetic nephropathy and takes
part in a joint renal-diabetic clinic at University Hospital Lewisham.
Locations
Click on address for links:
London Bridge:
Outpatient Clinic:
HCA Diagnostics Centre, The Shard, St Thomas Street, London SE1 9BS
Inpatients:
London Bridge Hospital, 27 Tooley Street, London, SE1 2PR
Chelsea:
Outpatient Clinic and Inpatients:
The Lister Hospital, Chelsea Bridge Road,London SW1W 8RH
Clinic Times:
The Shard
(6th Floor Southwark Suite)
Mondays 1730-2000
Tuesdays 1730-2000
Lister Hospital
(Arygle Suite)
Wednesdays 1800-2000
Appointments and contact
For new private patient appointments please call HCA contact centre
+44(0) 20 7079 4344
Or online via Doctify
Dr David Game | Nephrologist in London - Doctify
Queries to Vivian Benye
+44 7733518816
See Fees and contacts tab